Methotrexate Tablets contain 2.5 mg of Methotrexate.
Pharmacology: Pharmacodynamics: Methotrexate (4-amino-10 methyl folic acid) is an antimetabolite and an analogue of folic acid. The drug enters the cells via an active transport system for reduced folates and, due to a relatively irreversible binding, methotrexate inhibits dihydrofolic acid reductase. Dihydrofolates must be reduced to tetrahydrofolates by this enzyme before they can be utilized as carriers of one-carbon groups in the synthesis of purine nucleotides and thymidylate. Therefore, methotrexate interferes with DNA synthesis, repair, and cellular replication. The affinity of dihydrofolate reductase for methotrexate is far greater than its affinity for folic or dihydrofolic acid and, therefore, even very large amounts of folic acid given simultaneously will not reverse the effects of methotrexate. The drug seems also to cause an increase in intracellular deoxyadenosine triphosphate, which is thought to inhibit ribonucleotide reduction and polynucleotide ligase, an enzyme concerned in DNA synthesis and repair.
Actively proliferating tissues, such as malignant cells, bone marrow, fetal cells, buccal and intestinal mucosa, spermatogonia, and cells of the urinary bladder are in general more sensitive to this effect of methotrexate. Due to increased cellular proliferation methotrexate may impair malignant growth without irreversible damage to normal tissues.
In psoriasis, the rate of production of epithelial cells in the skin is greatly increased over normal skin. This differential in proliferation rates is the basis for the use of methotrexate to control the psoriatic process.
Methotrexate in high doses, followed by folinic acid rescue, is used as a part of the treatment of patients with non-metastatic osteosarcoma. The original rationale for high-dose methotrexate therapy was based on the concept of selective rescue of normal tissues by folinic acid. More recent evidence suggests that high-dose methotrexate may also overcome methotrexate resistance caused by impaired active transport, decreased affinity of dihydrofolic acid reductase for methotrexate, increased levels of dihydrofolic acid reductase resulting from gene amplification, or decreased polyglutamation of methotrexate. The actual mechanism of action is unknown.
In the treatment of rheumatoid arthritis, the precise mechanism of action of methotrexate is unknown. Methotrexate is used as monotherapy, as well as in combination with other interventions. Methotrexate is classified as a disease modifying antirheumatic drug (DMARD) in the treatment of rheumatoid arthritis.
Pharmacokinetics: Absorption: Rapid and complete absorption is achieved following intramuscular administration and peak serum levels are reached within 0.25 - 2 hrs. Oral absorption appears to be dose-dependent. Peak serum levels are reached within one to five hours. At doses of 30 mg/m2 or less, methotrexate is generally well absorbed with a mean bioavailability of about 60%. The absorption of doses greater than 80 mg/m2 is significantly less, possibly due to a saturation effect. Variability in methotrexate absorption has been however detected in subjects receiving oral treatment due to drug-induced epithelial denudation, motility changes and alterations in intestinal flora. Peak serum levels achievable following oral administration are slightly lower than those detected after intramuscular injection.
In leukemic pediatric patients, oral absorption of methotrexate also appears to be dose-dependent and has been reported to vary widely (23% to 95%). A twenty-fold difference between highest and lowest peak levels (Cmax: 0.11 to 2.3 micromolar after a 20 mg/m2 dose) has been reported. Significant interindividual variability has also been noted in time-to-peak concentration (Tmax 0.67 to 4 hours after a 15 mg/m2 dose) and fraction of dose absorbed. The absorption of doses greater than 40 mg/m2 has been reported to be significantly less than that of lower doses.
Distribution: After intravenous administration, the initial volume of distribution is approximately 0.18 L/kg (18% of body weight) and steady-state volume of distribution is approximately 0.4 to 0.8 L/kg (40% to 80% of body weight). Methotrexate competes with reduced folates for active transport across cell membranes by means of a single carrier-mediated active transport process. At serum concentrations greater than 100 micromolar, passive diffusion becomes a major pathway by which effective intracellular concentrations can be achieved. Methotrexate in serum is approximately 50% reversibly bound to protein.
Methotrexate is widely distributed into body tissues with highest concentrations in the kidneys, gallbladder, spleen, liver and skin. Methotrexate does not penetrate the blood-cerebrospinal fluid barrier in therapeutic amounts when given orally.
Small amounts have been detected in saliva and breast milk.
The drug crosses the placental barrier. The drug enters slowly into third-space collections of fluid, such as pleural effusions, ascites and marked tissue edemas.
In dogs, synovial fluid concentrations after oral dosing were higher in inflamed than uninflamed joints. Although salicylates did not interfere with this penetration, prior prednisone treatment reduced penetration into inflamed joints to the level of normal joints.
Metabolism: At low doses, methotrexate does not appear to undergo significant metabolism; following high dose therapy methotrexate undergoes hepatic and intracellular metabolism to polyglutamated forms that can be converted back to methotrexate by hydrolase enzymes. These polyglutamates act as inhibitors of dihydrofolate reductase and thymidylate synthetase. Small amounts of methotrexate polyglutamates may remain in tissues for extended periods. The retention and prolonged drug action of these active metabolites vary among different cells, tissues, and tumors. A small amount of metabolism to 7-hydroxymethotrexate may occur at doses commonly prescribed. Accumulation of this metabolite may become significant at the high doses used in osteogenic sarcoma. The aqueous solubility of 7-hydroxymethotrexate is 3- to 5-fold lower than the parent compound. Methotrexate is partially metabolized by intestinal flora after oral administration.
Half-life - The terminal half-life reported for methotrexate is approximately three to ten hours for patients receiving treatment for psoriasis, rheumatoid arthritis or low dose antineoplastic therapy (less than 30 mg/m2). For patients receiving high doses of methotrexate, the terminal half-life is 8 to 15 hours.
In pediatric patients receiving methotrexate for acute lymphocytic leukemia (6.3 to 30 mg/m2), the terminal half-life has been reported to range from 0.7 to 5.8 hours.
Elimination: Renal excretion is the primary route of elimination and is dependent upon dosage and route of administration. There is limited biliary excretion amounting to 10% or less of the administered dose. Enterohepatic recirculation of methotrexate has been proposed.
Renal excretion occurs by glomerular filtration and active tubular secretion. Nonlinear elimination due to saturation of renal tubular reabsorption has been observed in psoriatic patients at doses between 7.5 and 30 mg. Impaired renal function, as well as concurrent use of drugs, such as weak organic acids that also undergo tubular secretion, can markedly increase methotrexate serum levels. Excellent correlation has been reported between methotrexate clearance and endogenous creatinine clearance.
Total methotrexate clearance averages 12 L/h, but clearance rates vary widely and are generally decreased at higher doses. Delayed drug clearance has been identified as one of the major factors responsible for methotrexate toxicity. It has been postulated that the toxicity of methotrexate for normal tissues is more dependent upon the duration of exposure to the drug rather than the peak level achieved. When a patient has delayed drug elimination due to compromised renal function, a third space effusion, or other causes, methotrexate serum concentrations may remain elevated for prolonged periods.
The potential for toxicity from high dose regimens or delayed excretion is reduced by the administration of folinic acid during the final phase of methotrexate plasma elimination.
Effects of food: The bioavailability of orally administered methotrexate is not reduced by food and methotrexate may be administered without regard to meals.
Toxicology: Preclinical safety data: The intraperitoneal LD50 of methotrexate was 94 and 6 to 25 mg/kg for mice and rats, respectively. The oral LD50 of the compound in rats was 180 mg/kg. The tolerance to methotrexate in mice increased with age. In dogs, the intravenous dose of 50 mg/kg was lethal. The main targets after a single dose were the hemolymphopoietic system and gastrointestinal (GI) tract.
The toxic effects after repeated administration of methotrexate were investigated in mice and rats. The main targets of methotrexate in the previously mentioned animal species were the hemolymphopoietic system, GI tract, lung, liver, kidney, testes, and skin. The tolerance of mice to chronic methotrexate doses increased with age.
Methotrexate has been evaluated in a number of animal studies for carcinogenic potential with inconclusive results. Although there is evidence that methotrexate causes chromosomal damage to animal somatic cells and human bone marrow cells, the clinical significance remains uncertain.
The following are representative indications. Locally approved indications may differ.
Methotrexate is a cytotoxic drug used for antineoplastic chemotherapy and in certain nonmalignant conditions.
Anti-neoplastic Chemotherapy: Methotrexate is indicated for the treatment of gestational choriocarcinoma, and in patients with chorioadenoma destruens and hydatidiform mole.
Methotrexate is indicated for the palliation of acute lymphocytic leukemia. It is also indicated in the treatment and prophylaxis of meningeal leukemia. Greatest effect has been observed in palliation of acute lymphoblastic (stem-cell) leukemias in children. In combination with other anticancer drugs or suitable agents Methotrexate may be used for induction of remission, but it is most commonly used, as described in the monograph, in the maintenance of induced remissions.
Methotrexate may be used alone or in combination with other anticancer agents in the management of breast cancer, epidermoid cancers of the head and neck, and lung cancer, particularly squamous cells and small cell types.
Methotrexate is also effective in the treatment of the advanced stages (III and IV, Peters Staging System) of lymphosarcoma, particularly in those cases in children; and in advanced cases of mycosis fungoides.
Psoriasis Chemotherapy (See Precautions): Because of high risk attending its use, Methotrexate is only indicated in the symptomatic control of severe, recalcitrant, disabling psoriasis which is not adequately responsive to other forms of therapy, but only when the diagnosis has been established, as by biopsy and/or after dermatologic consultation.
Rheumatoid arthritis.
Anti-neoplastic chemotherapy: Oral administration in tablet form is often preferred since absorption is rapid and effective serum levels are obtained.
Choriocarcinoma and similar trophoblastic diseases: Methotrexate is administered orally in doses of 15 to 30 mg daily for a 5 day course. Such courses are usually repeated for 3 to 5 times as required, with rest periods of one or more weeks interposed between courses, until any manifesting toxic symptoms subside. The effectiveness of therapy is ordinarily evaluated by 24 hour quantitative analysis of urinary chorionic gonadotropin hormone (CGH), which should return to normal or less than 50 IU/24 hr, usually after the 3rd or 4th course and usually be followed by a complete resolution of measurable lesions in 4 to 6 weeks. One to two courses of Methotrexate after normalization of CGH is usually recommended. Before each course of the drug, careful clinical assessment is essential. Cyclic combination therapy of Methotrexate with other antitumor drugs has been reported as being useful.
Since hydatidiform mole may precede or be followed by choriocarcinoma, prophylactic chemotherapy with Methotrexate has been recommended. Chorioadenoma destruens is considered to be an invasive form of hydatidiform mole. Methotrexate is administered in these disease states in doses similar to those recommended for choriocarcinoma.
Leukemia: acute lymphatic (lymphoblastic) leukemia in children and young adolescents is the most responsive to present day chemotherapy. In young adults and older patients, clinical remission is more difficult to obtain and early relapse is more common. In chronic lymphatic leukemia, the prognosis for adequate response is less encouraging.
Methotrexate alone or in combination with steroids was used initially for induction of remission of lymphoblastic leukemias. More recently corticosteroid therapy in combination with other antileukemic drugs or in cyclic combinations with Methotrexate included appear to produce rapid and effective remissions. When used for induction, Methotrexate alone or in combination with other agents appears to be the drug of choice for securing maintenance of drug induced remissions. When remission is achieved and supportive care has produced general clinical improvement, maintenance therapy is initiated, as follows: Methotrexate is administered 2 times weekly by mouth. If and when relapse does occur, reinduction of remission can again usually be obtained by repeating the initial induction regimen. Various experts have recently introduced a variety of dosage schedules for both induction and maintenance of remission with various combinations of alkylating and antifolic agents. Multiple drug therapy with several agents, including Methotrexate given concomitantly is gaining increasing support in both the acute and chronic forms of leukemia. The physician should familiarize himself with the new advances in antileukemic therapy.
Acute granulocytic leukemia is rare in children but common in adults. This form of leukemia responds poorly to chemotherapy and remissions are short with relapses common, and resistance to therapy develops rapidly.
Meningeal leukemia: Patients with leukemia are subject to leukemic invasion of the central nervous system. This may manifest characteristic signs or symptoms or may remain silent and be diagnosed only by examination of the cerebrospinal fluid which contains leukemic cells in such cases. Therefore, the CSF should be examined in all leukemic patients.
For the treatment of meningeal leukemia, Methotrexate is given at intervals of 2 to 5 days. Methotrexate is administered until the cell count of the cerebrospinal fluid returns to normal. At this point one additional dose is advisable.
For prophylaxis against meningeal leukemia, the dosage is the same as for treatment except for the intervals of administration. On this subject, it is advisable for the physician to consult the medical literature.
Lymphomas: In Burkitt's Tumor, Stages I-II, Methotrexate has produced prolonged remissions in some cases. Recommended dosage is 10 to 25 mg per day orally for 4 to 8 days. In stage III, Methotrexate is commonly given concomitantly with other antitumor agents. Treatment in all stages usually consists of several courses of the drug interposed with 7 to 10 day rest periods. Lymphosarcomas in Stage III may respond to combined drug therapy with Methotrexate given in doses of 0.625 mg to 2.5 mg/kg daily. Hodgkin's Disease responds poorly to Methotrexate and to most types of chemotherapy.
Mycosis fungoides (cutaneous T cell lymphoma): Therapy with methotrexate as a single agent appears to produce clinical remission in one half of the cases treated. Dosage is usually 2.5 to 10 mg daily by mouth for weeks or months. Dose levels of drug and adjustment of dose regimen by reduction or cessation of drug are guided by patient response and hematologic monitoring.
Psoriasis Chemotherapy: The patient should be fully informed of the risks involved and should be under constant supervision of the physician.
Assessment of renal function, liver function, and blood elements should be made by history, physical examination, and laboratory tests (such as CBC, urinalysis, serum creatinine, liver function studies, and liver biopsy if indicated) before beginning Methotrexate, periodically during Methotrexate therapy, and before reinstituting Methotrexate therapy after a rest period. Appropriate steps should be taken to avoid conception during and for at least eight weeks following Methotrexate therapy.
There are three commonly used general types of dosage schedules: 1. weekly oral intermittent large doses; 2. divided dose intermittent oral schedule over a 36 hour period; 3. daily oral with a rest period.
All schedules should be continually tailored to the individual patient. Dose schedules cited as follows pertain to an average 70 kg adult. An initial test dose one week prior to initiation of therapy is recommended to detect any idiosyncrasy.
Recommended starting dose schedules: 1. Weekly single oral: 10-25 mg per week until adequate response is achieved. With this dosage schedule, 50 mg per week should ordinarily not be exceeded.
2. Divided oral dose schedule: 2.5 mg at 12 hour intervals for three doses or at 8 hour intervals for four doses each week. With this dosage schedule, 30 mg per week should not be exceeded.
3. Daily oral dose schedule: 2.5 mg daily for five days followed by at least a two day rest period. With this dosage schedule; 6.25 mg per day should not be exceeded.
SPECIAL NOTE: Available data suggest that schedule 3 may carry an increased risk of serious liver pathology.
Dosages in each schedule may be gradually adjusted to achieve optimal clinical response, but not to exceed the maximum stated for each schedule.
Once optimal clinical response has been achieved, each dosage schedule should be reduced to the lowest possible amount of drug and to the longest possible rest period. The use of Methotrexate may permit the return to conventional topical therapy, which should be encouraged.
Rheumatoid arthritis (RA): 1. Single oral doses of 7.5 to 20 mg once weekly.
2. Divided oral doses of 2.5 to 7.5 mg every 12 hours for three doses, repeated weekly.
A total weekly dose 20 mg should not be exceeded. Once optimal clinical response has been achieved, dosing should be reduced to the lowest possible effective dose. The optimal duration of therapy is unknown; limited data from long term studies indicate that the initial clinical improvement is maintained for at least 2 years with continued therapy.
Pediatric use: Safety and effectiveness in pediatric patients have been established only in cancer chemotherapy.
Geriatric use: Fatal toxicities related to inadvertent daily rather than weekly dosing have been reported, particularly in elderly patients. It should be emphasized to the patient that the recommended dose is taken weekly for psoriasis.
Due to diminished hepatic and renal function as well as decreased folate stores in this population, relatively low doses (especially in RA and psoriasis indications) should be considered and these patients should be closely monitored for early signs of toxicity (see Precautions).
In post-marketing experience, overdose with methotrexate has generally occurred with oral administration.
Reports of oral overdose indicate accidental daily administration instead of weekly (single or divided doses). Symptoms commonly reported following oral overdose include those symptoms and signs reported at pharmacologic doses, particularly hematologic and gastrointestinal reactions. For example, leukopenia, thrombocytopenia, anemia, pancytopenia, bone marrow suppression, mucositis, stomatitis, oral ulceration, nausea, vomiting, gastrointestinal ulceration, gastrointestinal bleeding. In some cases, no symptoms were reported. There have been reports of death following chronic overdose in the self administered dosage for rheumatoid arthritis and psoriasis (see Dosage & Administration and Precautions). In these cases, events, such as sepsis or septic shock, renal failure, and aplastic anemia were also reported.
Recommended treatment: Folinic acid is indicated to diminish the toxicity and counteract the effect of inadvertently administered overdoses of methotrexate. Folinic acid administration should begin as promptly as possible. As the time interval between methotrexate administration and leucovorin initiation increases, the effectiveness of folinic acid in counteracting toxicity decreases. Monitoring of the serum methotrexate concentration is essential in determining the optimal dose and duration of treatment with folinic acid.
In cases of massive overdose, hydration and urinary alkalization may be necessary to prevent the precipitation of methotrexate and/or its metabolites in the renal tubules. Neither standard hemodialysis nor peritoneal dialysis has been shown to improve methotrexate elimination. However, effective clearance of methotrexate has been reported with acute, intermittent hemodialysis using a high-flux dialyzer.
Hypersensitivity to methotrexate or any excipients in the formulation.
Breast feeding.
Severe renal impairment.
Applies to patients with psoriasis or rheumatoid arthritis only: Alcoholism, alcoholic liver disease, or other chronic liver disease.
Overt or laboratory evidence of immunodeficiency syndromes.
Preexisting blood dyscrasias, such as bone marrow hypoplasia, leukopenia, thrombocytopenia, or significant anemia.
Pregnancy.
General: Because of the possibility of serious toxic reactions (which can be fatal), methotrexate should be used only in neoplastic diseases (as indicated), or in patients with severe, recalcitrant, disabling psoriasis or rheumatoid arthritis that is not adequately responsive to other forms of therapy. The patient should be informed by the physician of the risks involved and should be under a physician's constant supervision. Refer to Use in the Elderly and Use in Children as follows for specific warnings.
It should be emphasized to the patient treated for rheumatoid arthritis and psoriasis that the recommended dose must be taken weekly, and that mistaken daily use of the recommended dose has led to fatal toxicity (see Dosage & Administration and Overdosage).
Methotrexate has been reported to cause fetal death and/or congenital anomalies. It is not recommended for the treatment of neoplastic diseases in women of childbearing potential.
Like other cytotoxic drugs, methotrexate may induce "tumor lysis syndrome" in patients with rapidly growing tumors. Appropriate supportive and pharmacologic measures may prevent or alleviate this complication.
Severe, occasionally fatal, skin reactions such as Stevens-Johnson Syndrome, toxic epidermal necrolysis (Lyell's syndrome), have been reported following single or multiple doses of methotrexate.
Methotrexate causes hepatotoxicity, liver fibrosis, and cirrhosis, but generally only after prolonged use. Acutely, liver enzyme elevations are frequently seen. These are usually transient and asymptomatic, and do not appear predictive of subsequent hepatic disease. Liver biopsy after sustained use often shows histologic changes, and fibrosis and cirrhosis have been reported; these latter lesions may not be preceded by symptoms or abnormal liver function tests in the psoriasis population. Periodic liver biopsies are usually recommended for psoriatic patients who are under long-term treatment. Persistent abnormalities in liver function tests may precede appearance of fibrosis or cirrhosis in the rheumatoid arthritis population.
Methotrexate has caused reactivation of hepatitis B infection or worsening of hepatitis C infections, in some cases resulting in death. Some cases of hepatitis B reactivation have occurred after discontinuation of methotrexate. Clinical and laboratory evaluation should be performed to evaluate preexisting liver disease in patients with prior hepatitis B or C infections. Based on these evaluations, treatment with methotrexate may not be appropriate for some patients.
Methotrexate-induced lung disease, including acute or chronic interstitial pneumonitis and pleural effusion, may occur at any time during therapy and has been reported at low doses. It is not always fully reversible, and fatalities have been reported. Rheumatoid arthritis patients are at risk to develop rheumatoid lung disease, which is often associated with interstitial pulmonary disease. Methotrexate may exacerbate this underlying lung disease. Pulmonary symptoms (especially a dry, nonproductive cough) may require interruption of treatment and careful investigation.
Diarrhea and ulcerative stomatitis require interruption of therapy, otherwise, hemorrhagic enteritis and death from intestinal perforation may occur. Methotrexate should be used with extreme caution in the presence of peptic ulcer disease or ulcerative colitis.
Methotrexate given concomitantly with radiotherapy may increase the risk of soft tissue necrosis and osteonecrosis.
Methotrexate exits slowly from third space compartments (e.g., pleural effusions, ascites). This results in a prolonged terminal half-life and unexpected toxicity. In patients with significant third space accumulations, it is advisable to evacuate the fluid before treatment and to monitor plasma methotrexate levels.
Methotrexate therapy in patients with impaired renal function should be undertaken with extreme caution, and at reduced doses, because impairment of renal function will decrease methotrexate elimination.
It is necessary to follow patients on methotrexate closely. Methotrexate has the potential for serious toxicity. Toxic effects may be related in frequency and severity to dose or frequency of administration, but has been seen at all doses and can occur at any time during therapy. Most adverse reactions are reversible if detected early. When such reactions do occur, the dosing should be reduced or discontinued and appropriate corrective measures should be taken. If methotrexate therapy is reinstituted, it should be carried out with caution, with adequate consideration of further need for the drug, and with increased alertness as to possible recurrence of toxicity.
Patients should be informed of the potential benefits and risks in the use of methotrexate (including the early signs and symptoms of toxicity), the need to see their physician promptly if they occur, and of the need for close follow-up, including periodic laboratory tests, to monitor toxicity.
The use of methotrexate high-dose regimens (≥500 mg/m2) recommended for osteosarcoma requires meticulous care (see Dosage & Administration). High dosing regimens for other neoplastic diseases are investigational and a therapeutic advantage has not been established.
Malignant lymphomas, may occur in patients receiving low-dose methotrexate. These lymphomas may regress following withdrawal of methotrexate without requiring treatment.
Folate deficiency states may increase methotrexate toxicity.
Organ system toxicity: Gastrointestinal: If vomiting, diarrhea, or stomatitis occur, resulting in dehydration, supportive therapy should be instituted and methotrexate discontinuation until recovery occurs, should be considered.
Hematologic: Methotrexate can suppress hematopoiesis and cause anemia, aplastic anemia, pancytopenia, leukopenia, neutropenia, and/or thrombocytopenia. Methotrexate should be used with caution in patients with preexisting hematopoietic impairment (see Interactions). The nadir of circulating leukocytes, neutrophils and platelets usually occurs between 5 to 13 days after an IV bolus dose (with recovery between 14 to 28 days). Leukocytes and neutrophils may occasionally show two depressions, the first occurring in 4 to 7 days and a second nadir after 12 to 21 days, followed by recovery. Clinical sequelae such as fever, infections and hemorrhage from various sites may be expected. In the treatment of neoplastic diseases, methotrexate should be continued only if the potential benefit outweighs the risk of severe myelosuppression. In psoriasis and rheumatoid arthritis, methotrexate should be stopped immediately if there is a significant drop in blood cell counts.
Hepatic: Methotrexate has the potential for acute hepatitis and chronic (fibrosis and cirrhosis) hepatotoxicity. Chronic toxicity is potentially fatal; it generally has occurred after prolonged use (generally two years or more) and after a total cumulative dose of at least 1.5 grams. In studies in psoriatic patients, hepatotoxicity appeared to be a function of total cumulative dose and appeared to be enhanced by alcoholism, obesity, diabetes and advanced age.
Transient abnormalities of liver parameters are observed frequently after methotrexate administration and are usually not a reason for modification of methotrexate therapy. Persistent liver abnormalities, and/or decrease of serum albumin may be indicators of serious liver toxicity.
In psoriasis, liver damage and function tests, including serum albumin and prothrombin time, should be performed several times prior to dosing. Liver function tests are often normal in developing fibrosis or cirrhosis. These lesions may be detectable only by biopsy. It is recommended to obtain a liver biopsy at: 1) before start of therapy or shortly after initiation of therapy (2-4 months); 2) after a total cumulative dose of 1.5 grams; and 3) after each additional 1.0 to 1.5 grams. In case of moderate fibrosis or any cirrhosis, discontinue the drug; mild fibrosis normally suggests a repeat biopsy in 6 months. Milder histologic findings, such as fatty change and low grade portal inflammation are relatively common before the start of therapy. Although these mild changes are usually not a reason to avoid or discontinue methotrexate therapy, the drug should be used with caution.
In rheumatoid arthritis, age at first use of methotrexate and duration of therapy have been reported as risk factors for hepatotoxicity. Persistent abnormalities in liver function tests may precede appearance of fibrosis or cirrhosis in the rheumatoid population. Liver function tests should be performed at baseline and at 4 to 8 week intervals in patients receiving methotrexate for rheumatoid arthritis. Pretreatment liver biopsy should be performed for patients with a history of excessive alcohol consumption, persistently abnormal baseline liver function test values, or chronic hepatitis B or C infection. During therapy, liver biopsy should be performed if there are persistent liver function test abnormalities, or there is a decrease in serum albumin below the normal range (in the setting of well controlled rheumatoid arthritis).
If the results of a liver biopsy show mild changes (Roenigk grades I, II, IIIa), methotrexate may be continued and the patient monitored according to the recommendations listed previously. Methotrexate should be discontinued in any patient who displays persistently abnormal liver function tests and refuses liver biopsy, or in any patient whose liver biopsy shows moderate to severe changes (Roenigk grade IIIb or IV).
Infection or immunologic states: Methotrexate should be used with extreme caution in the presence of active infection, and is usually contraindicated in patients with overt or laboratory evidence of immunodeficiency syndromes.
Potentially fatal opportunistic infections, including Pneumocystis carinii pneumonia, may occur with methotrexate therapy. When a patient presents with pulmonary symptoms, the possibility of Pneumocystis carinii pneumonia should be considered.
Immunization: Vaccinations may be less immunogenic when given during methotrexate therapy. Immunization with live virus vaccines is generally not recommended. There have been reports of disseminated vaccinia infections after smallpox immunization in patients receiving methotrexate therapy.
Neurologic: There have been reports of leukoencephalopathy following intravenous administration of methotrexate to patients who have had craniospinal irradiation. Refer to Use in Children as follows for specific warnings. Symptomatic patients were commonly noted to have leukoencephalopathy and/or microangiopathic calcifications on diagnostic imaging studies.
Chronic leukoencephalopathy has also been reported in patients who received repeated doses of high-dose methotrexate with folinic acid rescue even without cranial irradiation. There are also reports of leukoencephalopathy in patients who received oral methotrexate.
Discontinuation of methotrexate does not always result in complete recovery.
A transient acute neurologic syndrome has been observed in patients treated with high dosing regimens. Manifestations of this neurologic syndrome may include behavioral abnormalities, focal sensorimotor signs, including transient blindness, and abnormal reflexes. The exact cause is unknown.
Cases of severe neurological adverse reactions that ranged from headache to paralysis, coma and stroke-like episodes have been reported mostly in juveniles and adolescents given methotrexate in combination with cytarabine.
Pulmonary: Pulmonary signs and symptoms, e.g., a dry nonproductive cough, fever, cough, chest pain, dyspnea, hypoxemia, and an infiltrate on chest X-ray, or a nonspecific pneumonitis occurring during methotrexate therapy, may be indicative of a potentially dangerous lesion and require interruption of treatment and careful investigation. Methotrexate induced pneumonitis can occur at all doses. Infection (including pneumonia) needs to be excluded.
Renal: Methotrexate may cause renal damage that may lead to acute renal failure. Close attention to renal function including adequate hydration, urine alkalinization, and measurement of serum methotrexate and renal function are recommended.
Concomitant use of proton pump inhibitors (PPIs) and high dose methotrexate should be avoided, especially in patients with renal impairment.
Skin: Severe, occasionally fatal, dermatologic reactions, including toxic epidermal necrolysis (Lyell's Syndrome), Stevens-Johnson syndrome, and erythema multiforme, have been reported within days of oral methotrexate administration.
Lesions of psoriasis may be aggravated by concomitant exposure to ultraviolet radiation. Radiation dermatitis and sunburn may be "recalled" by the use of methotrexate.
Laboratory monitoring: General: Patients undergoing methotrexate therapy should be closely monitored so that toxic effects are detected promptly.
Baseline assessment should include a complete blood count with differential and platelet counts; hepatic enzymes, hepatitis B or C infection testing, renal function tests; and a chest X-ray.
During therapy of rheumatoid arthritis and psoriasis, monitoring of the following parameters is recommended: hematology at least monthly, hepatic enzyme levels and renal function every 1 to 2 months. More frequent monitoring is usually indicated during antineoplastic therapy. During initial or change in dosing, or during periods of increased risk of elevated methotrexate blood levels (e.g., dehydration), more frequent monitoring may also be indicated.
Pulmonary function tests: Pulmonary function tests may be useful if lung disease (e.g., interstitial pneumonitis) is suspected, especially if baseline measurements are available.
Methotrexate level: Serum methotrexate level monitoring can significantly reduce toxicity and mortality by allowing the adjustment of methotrexate dosing and the implementation of appropriate rescue measures.
Patients subject to the following conditions are predisposed to developing elevated or prolonged methotrexate levels and benefit from routine monitoring of levels: e.g., pleural effusion, ascites, gastrointestinal tract obstruction, previous cisplatin therapy, dehydration, aciduria, impaired renal function.
Some patients may have delayed methotrexate clearance in the absence of these features. It is important that patients be identified within 48 hours since methotrexate toxicity may not be reversible if adequate folinic acid rescue is delayed for more than 42 to 48 hours.
The method of monitoring methotrexate concentrations varies from institution to institution. Monitoring of methotrexate concentrations should include determination of a methotrexate level at 24, 48, or 72 hours, and assessment of the rate of decline in methotrexate concentrations (to determine how long to continue folinic acid rescue).
Effects on ability to drive and use machines: Some of the effects reported in Adverse Reactions (e.g., dizziness, fatigue) may have an influence on the ability to drive and use machines.
Use in Children: Safety and effectiveness in pediatric patients have been established only in cancer chemotherapy.
Use in the Elderly: Fatal toxicities related to inadvertent daily rather than weekly dosing have been reported, particularly in elderly patients. It should be emphasized to the patient that the recommended dose is taken weekly for rheumatoid arthritis and psoriasis (see Dosage & Administration).
Fertility: Methotrexate has been reported to cause impairment of fertility, oligospermia and menstrual dysfunction in humans, during and for a short period after cessation of therapy.
Pregnancy: Methotrexate can cause fetal death, embryotoxicity, abortion, or teratogenic effects when administered to a pregnant woman. Methotrexate is contraindicated in pregnant patients with psoriasis or rheumatoid arthritis.
Women of childbearing potential should not be started on methotrexate until pregnancy is excluded and should be fully counseled on the serious risk to the fetus should they become pregnant while undergoing treatment. Pregnancy should be avoided if either partner is receiving methotrexate.
The optimal time interval between the cessation of methotrexate treatment of either partner and pregnancy has not been clearly established. Published literature recommendations for time intervals vary from 3 months to one year.
The risk of effects on reproduction should be discussed with both male and female patients taking methotrexate.
Lactation: Methotrexate has been detected in human breast milk and is contraindicated during breast feeding.
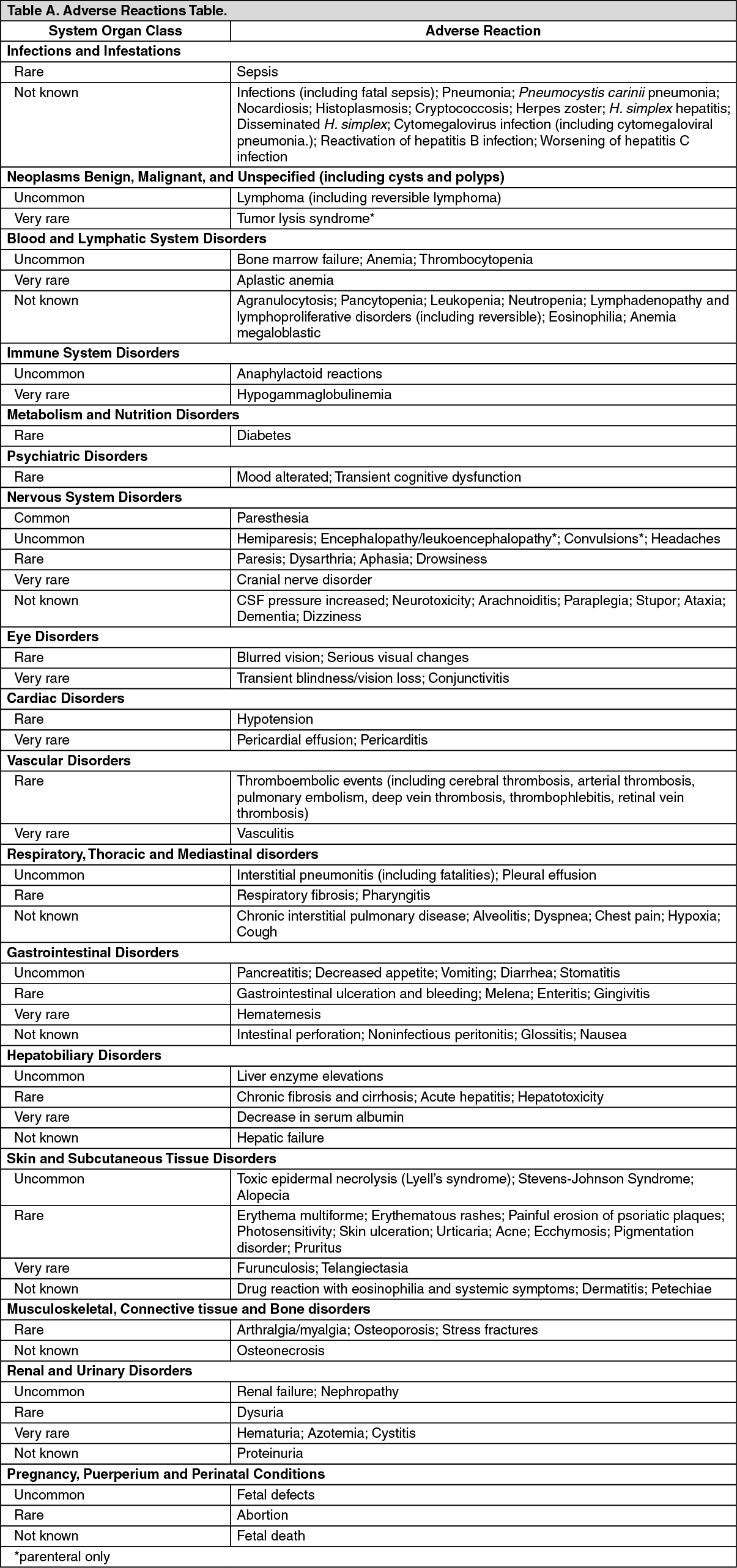
In general, the incidence and severity of adverse drug reactions are related to dose and frequency of administration. Relevant sections should be consulted when looking for information about adverse reactions with methotrexate.
The most frequently reported adverse reactions include ulcerative stomatitis, leukopenia, nausea, and abdominal distress. Other frequently reported adverse effects are malaise, undue fatigue, chills and fever, dizziness, and decreased resistance to infection. Ulcerations of the oral mucosa are usually the earliest signs of toxicity.
Other adverse reactions that have been reported with methotrexate are listed as follows by organ system and by frequency. In the oncology setting, concomitant treatment and the underlying disease make specific attribution of a reaction to methotrexate difficult. See Precautions for specific reference to medically important and long term events including those following long term treatment or high cumulative doses (e.g., hepatic toxicity).
Frequency categories are defined as: Very common (≥1/10), Common (≥1/100 to <1/10), Uncommon (≥1/1,000 to <1/100), Rare (≥1/10,000 to <1/1,000), Very rare (<1/10,000), Not known (cannot be estimated from the available data). (See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Chemotherapeutic agents: Enhancement of nephrotoxicity may be seen when high-dose methotrexate is administered in combination with a potentially nephrotoxic chemotherapeutic agent (e.g., cisplatin).
Cytarabine: Intrathecal methotrexate given concomitantly with IV cytarabine may increase the risk of severe neurologic adverse events such as headache, paralysis, coma and stroke-like episodes.
L-asparaginase: The administration of L-asparaginase has been reported to antagonize the effect of MTX.
Mercaptopurine: Methotrexate increases the plasma levels of mercaptopurine. Combination of methotrexate and mercaptopurine may therefore require dose adjustment.
Disease-modifying antirheumatic drug (DMARD) and Nonsteroidal Anti-inflammatory Drugs (NSAIDs): NSAIDs should not be administered prior to or concomitantly with the high doses of methotrexate such as used in the treatment of osteosarcoma. Concomitant administration of NSAIDs with high-dose methotrexate therapy has been reported to elevate and prolong serum methotrexate levels, resulting in deaths from severe hematologic (including bone marrow suppression and aplastic anemia) and gastrointestinal toxicity. NSAIDs and salicylates have been reported to reduce the tubular secretion of methotrexate in an animal model and may enhance its toxicity by increasing methotrexate levels. Therefore, caution should be used when they are administered concomitantly with lower doses of methotrexate.
In treating rheumatoid arthritis with methotrexate, aspirin, NSAIDs, and/or low dose steroids may be continued.
The possibility of increased toxicity with concomitant use of NSAIDs including salicylates has not been fully explored. Steroids may be reduced gradually in patients who respond to methotrexate. Despite the potential interactions, studies of methotrexate in patients with rheumatoid arthritis have usually included concurrent use of constant dosing regimens of NSAIDs, without difficulty. However, the methotrexate doses used in rheumatoid arthritis (7.5 to 15 mg/week) are somewhat lower than those used in psoriasis, and larger doses could lead to unexpected toxicity. Combined use of methotrexate with gold, penicillamine, hydroxychloroquine, sulfasalazine, has not been studied and may increase the incidence of adverse effects.
Proton pump inhibitors: Co-administration of proton pump inhibitors (PPIs) with methotrexate may decrease the clearance of methotrexate causing elevated methotrexate plasma levels with clinical signs and symptoms of methotrexate toxicity. Concomitant use of PPIs and high dose methotrexate should therefore be avoided, especially in patients with renal impairment.
Antibiotics: Ciprofloxacin: Renal tubular transport is diminished by ciprofloxacin; use of methotrexate with this drug should be carefully monitored.
Penicillins and sulfonamides: Penicillins and sulfonamides may reduce the renal clearance of methotrexate; hematologic and gastrointestinal toxicity has been observed in combination with high- and low-dose methotrexate.
Oral antibiotics: Oral antibiotics, such as tetracycline, chloramphenicol, and nonabsorbable broad spectrum antibiotics, may decrease intestinal absorption of methotrexate or interfere with the enterohepatic circulation by inhibiting bowel flora and suppressing metabolism of methotrexate by bacteria.
Trimethoprim/sulfamethoxazole has been reported rarely to increase bone marrow suppression in patients receiving methotrexate, probably by decreased tubular secretion and/or additive antifolate effect.
Concurrent use of the anti-protozoal pyrimethamine may increase the toxic effects of methotrexate because of an additive antifolate effect.
Hepatotoxic agents: The potential for increased hepatotoxicity when methotrexate is administered with other hepatotoxic agents has not been evaluated. However, hepatotoxicity has been reported in such cases. Therefore, patients receiving concomitant therapy with methotrexate and other potential hepatotoxic agents (e.g., leflunomide, azathioprine, sulfasalazine, retinoids) should be closely monitored for possible increased risk of hepatotoxicity.
Nitrous oxide anesthesia: The use of nitrous oxide anesthesia potentiates the effect of methotrexate on folate metabolism, yielding increased toxicity such as severe unpredictable myelosuppression and stomatitis. This effect can be reduced by the use of folinic acid rescue (see Dosage & Administration).
Probenecid: Renal tubular transport is diminished by probenecid; use of methotrexate with this drug should be carefully monitored.
Vitamins: Vitamin preparations containing folic acid or its derivatives may decrease responses to systemically administered methotrexate, however, folate deficiency states may increase methotrexate toxicity.
Amiodarone: Amiodarone administration to patients receiving methotrexate treatment for psoriasis has induced ulcerated skin lesions.
Drugs highly bound to plasma proteins: Methotrexate is partially bound to serum albumin, and toxicity may be increased because of displacement by other highly bound drugs, such as sulfonylureas, aminobenzoic acid, salicylates, phenylbutazone, phenytoin, sulfonamides, some antibiotics such as penicillins, tetracycline, pristinamycin, probenecid, and chloramphenicol.
Leflunomide: Methotrexate in combination with leflunomide may increase the risk of pancytopenia.
Psoralen plus ultraviolet light (PUVA) therapy: Skin cancer has been reported in few patients with psoriasis or mycosis fungoides (a cutaneous T-cell lymphoma) receiving a concomitant treatment with methotrexate plus PUVA therapy (methoxsalen and ultraviolet light).
Theophylline: Methotrexate may decrease the clearance of theophylline; theophylline levels should be monitored when used concurrently with methotrexate.
Diuretics: Bone marrow suppression and decreased folate levels have been described in the concomitant administration of triamterene and methotrexate.
Handling: Procedures for proper handling and disposal of anticancer drugs should be considered.
Tablet is non-divisible.
Store at room temperature below 30°C. Protect from light.
L04AX03 - methotrexate ; Belongs to the class of other immunosuppressants.
Methotrexate Pfizer tab 2.5 mg
100's;28's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image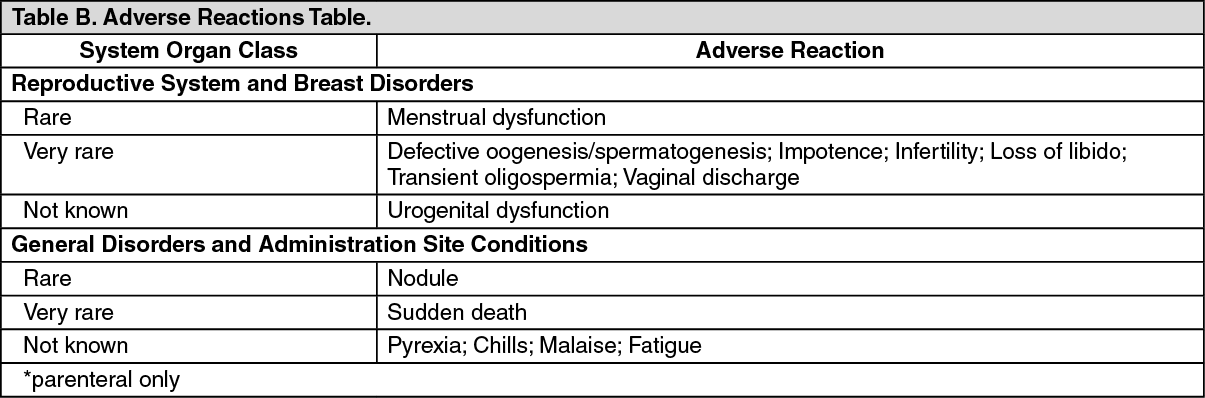 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
